

Thank you to our partners at CRISP Maryland for sharing this blog with the Civitas community!
CRISP, the state-designated Health Data Utility (HDU) of Maryland, is dedicated to supporting the Maryland health care community to appropriately share data to facilitate care, reduce costs, and improve health outcomes, and recognizes the value of services provided by community-based organizations across Maryland. In support of this mission, CRISP was excited to implement the Community and Clinical Data Initiative (CODI) Model with two community-based organizations (CBOs):
- MAC, Inc., an area agency on aging (AAA) on Maryland’s Eastern Shore who also acts as a community care hub for the AAAs across the state and provides a variety of programs and services that support older adults, and
- Meals on Wheels of Central Maryland (MOWCM), a home-delivered meals provider for five counties in the greater Baltimore area.
The Maryland CODI implementation aimed to improve older adult health by connecting community data about social needs and the programs or services that address those needs with clinical data.
Reducing Time and Costs – the HDU-centric CODI Approach
CODI is a model to harmonize community and clinical data to create a more complete picture of a person’s health for research, evaluation, quality improvement, and public health. The CODI Model is open source (free to use) and can help communities connect data across the siloed health information landscape to better understand the impact of community programs and services on population health outcomes.
The CODI model was originally pioneered by the Centers for Disease Control and Prevention with support from the Health Federally Funded Research and Development Center (Health FFRDC) operated by the MITRE Corporation and has been implemented previously in Colorado and North Carolina; these implementations used a distributed network approach that did not leverage existing health information exchange (HIE) or HDU infrastructure.
Based on lessons learned from these implementations, a new HDU-centric approach was piloted in Maryland by CRISP with support from the Administration for Community Living (ACL) and the Health FFRDC. This approach leveraged CRISP’s existing access to clinical data and its data sharing, ingestion, and reporting capabilities. This meant that minimal additional technology had to be built – accelerating the time to implementation and reducing the costs to maintain and sustain.
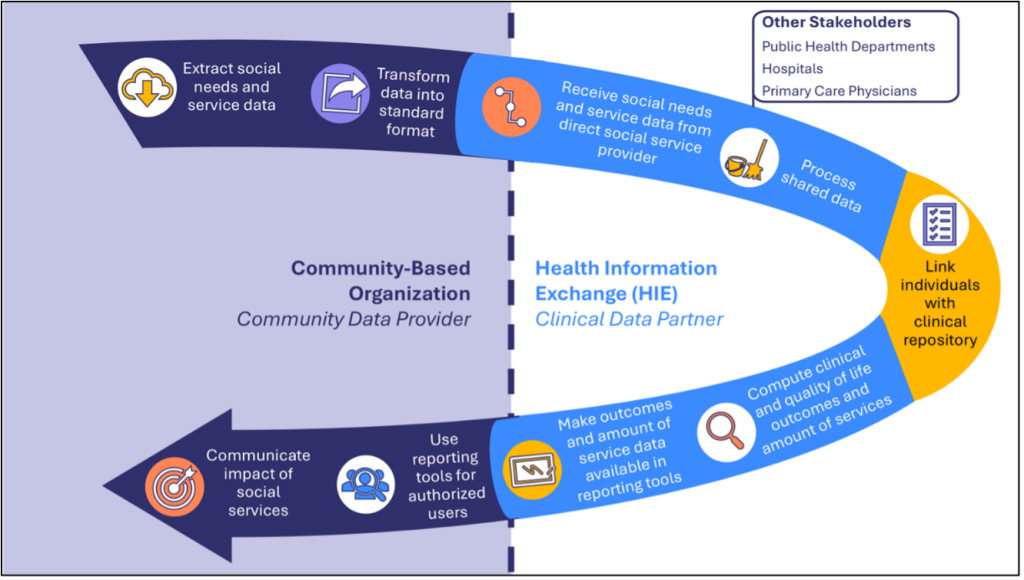
The figure below summarizes key steps in CODI Model implementation starting with data extraction and transformation by social service providers (e.g., CBOs), followed by the HDU receiving, processing, and linking data and computing outcomes, and finally the CBOs using the information provided by the HDU to communicate impact of services.
Addressing Barriers to Information Exchange Between CBOs and Clinical Organizations
Health care systems in Maryland are partnering with CBOs to help with screening, patient referrals, and delivering programs and services to address whole person health. CBOs play an essential role in maintaining and improving health by providing critical programs and services outside of a health care setting to people who have unmet food, housing, and other needs.
Unfortunately, most social service data are siloed at CBOs and are not easily accessed by other CBOs, health information organizations, health care providers, or payers. This also means that CBOs often struggle to close the loop with providers and demonstrate the impact of the services they provide. Demonstrating impact is difficult because CBOs cannot easily access clinical data to evaluate change in clinical outcome measures in the populations they serve.
The HDU-centric CODI approach addressed these challenges by offering a model for data sharing and use paired with open-source resources that support communities in implementing the model that can be customized to existing HDU infrastructure.

What Did Partners Hope to Gain by Implementing CODI in Maryland?
Defining clear value propositions for Maryland implementing partners was an important early activity. From CODI, CRISP hoped to strengthen partnerships with local CBOs, learn more about CBO workflows and desired reporting functionality, expand their catchment of social service data, and increase their use of clinical data for reporting. CBOs hoped to improve their data sharing capabilities, demonstrate innovation readiness, share more data with partner health systems via CRISP, and gain access to health outcomes data to demonstrate the value of their programs. At the conclusion of the CODI implementation in Maryland, each partner had achieved these goals.
Key Impacts in Maryland
The Maryland CODI implementation successfully resulted in the following key impacts:
1. Partners Gained Meaningful Insights from Connected Data
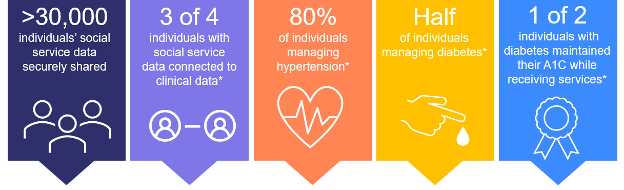
CBOs shared up to seven years of individual-level data about social needs and nine programs and services with CRISP. Using the shared data, CRISP linked participants to their clinical data and computed outcome measures about hypertension and diabetes. Key data points for this data journey are highlighted below.
This new information can be used by:
- CBOs to measure and advocate for the programs and services that drive meaningful change
- HDUs to recruit additional CBOs to begin submitting social service data and to demonstrate the potential value of connected data to health care partners
- Health care providers to improve understanding of which programs and services their patients are receiving and the resulting outcomes
- Policy makers to increase awareness of opportunities to improve health through strategic investment in services and programs
2. Partners Improved Technical Readiness
While preparing for data extraction and transformation, CBOs identified ways to improve data collection and implemented processes to improve data quality in their information systems. CBOs also gained an understanding of how their own information systems do and do not meet their functional needs. This makes CBOs better equipped to participate in data-sharing initiatives and support long-term goals. CBOs also implemented processes to extract data from three information systems, normalize it, and securely transmit it to CRISP.
CRISP expanded its capabilities to receive and process more detailed CBO data and compute three new health outcomes for clients served by CBOs (diabetes prevalence, diabetes control, and hypertension prevalence).
3. Partners Gained New and Stronger Relationships
The implementation fostered collaboration among CBOs, CRISP, and government entities, laying the groundwork for future initiatives and streamlined partnerships. CBOs shared that their strengthened relationships with CRISP and other partners were the most important gain from the CODI implementation.
What’s Next for CRISP and CODI?
CRISP is proud to continue to support and expand this work. In the spirit of the CODI model, CRISP will be operationalizing parts of what was learned in the CODI Pilot Model to the CRISP CBO Data Ingestion Model.
This CRISP ingestion model will allow CBO’s to easily send data to CRISP and expand the volume of CBO’s sending data. CRISP is also offering multiple ways CBOs can send data through either direct ingestion or from a “Roster” type submission. This allows flexibility based on the IT infrastructure the CBO has. As the volume of data grows CRISP will work to build reporting, both demographic and clinical, with the CBOs to ensure they can show their value to stakeholders.
Finally, CRISP plans to continue strengthening their relationships with CBO’s and expand this work to additional organizations that are interested. This will allow other CBO’s, government organizations and health care providers to connect and better understand the critical value that these CBO’s play in providing whole person care to the people of Maryland.
